
Background
Neonatal intestinal obstruction comprises many conditions, as obstruction may occur at any point in the gastrointestinal tract.
Even when restricting one’s focus to a single location, several variations of obstruction are possible. The general principles involved in managing intestinal obstruction are the same regardless of the patient population, from the newborn to the geriatric.
The following image depicts malrotation/volvulus.
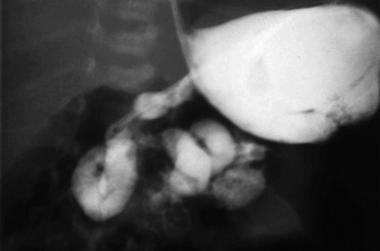
Intestinal obstruction in the newborn. Malrotation/volvulus. Note the spiral twist and the partial obstruction.
Intestinal obstruction occurs in approximately 1 in 2000 births
; hence, it is a frequent reason for pediatric surgical consultation.
Neonatal intestinal obstruction is suggested by the following features
:
Maternal
polyhydramnios
Feeding intolerance
Bilious emesis
Abdominal distention
Delayed passage of meconium
Absent transitional stools
Classic clinical signs of neonatal intestinal obstruction are vomiting, abdominal distention, and failure to pass meconium.
However, the infant’s clinical presentation is dependent on the anatomic level of the obstruction, as follows:
Foregut obstruction: Infants with foregut obstructions have difficulty swallowing, or they regurgitate or vomit gastric contents. Their abdominal examination may show localized distention, as in the left upper quadrant bulge that is typical of pyloric stenosis. Prolonged vomiting produces a characteristic electrolyte disturbance (hypokalemic metabolic alkalosis).
High (jejunal) obstruction: Babies with high (jejunal) obstructions vomit bilious succus entericus. Their abdominal evaluation reveals a scaphoid abdomen; however, a mass (distended bowel) may be palpable. Nasogastric output is generally voluminous, and characteristic electrolyte abnormalities (hyperkalemic metabolic acidosis) are present.
Distal small bowel or colonic obstruction: Babies with obstruction at these anatomic levels present with feeding intolerance and abdominal distention. If the diagnosis is delayed, feculent emesis may occur. Abdominal palpation may reveal a mass (intestinal duplication or intussusception). Plain radiographs show multiple dilated loops of bowel.
It is important to exercise clinical acumen. Conduct the following:
Obtain an accurate history.
Perform a careful, thorough physical examination.
Obtain radiographs that corroborate or refute the “working diagnosis.”
Once the correct diagnosis is ascertained, the surgeon can decide upon an appropriate intervention. Fortunately, the outlook for babies with intestinal obstruction is generally excellent.
Intestinal obstruction in a patient with peritonitis constitutes a surgical emergency; the presence of pain generally denotes ischemia. A loop of bowel may be twisted, creating a “closed loop” obstruction (see the image below). Because both limbs (loops) (afferent and efferent) are obstructed, there is no outlet and the bowel becomes massively distended. If the intraluminal pressure exceeds the blood pressure, perfusion ceases and the bowel dies. In “strangulation” obstruction, the mesentery is kinked and blood flow is impaired, causing ischemia and, ultimately, gangrene.

Intestinal obstruction in the newborn. Volvulus of a loop of intestine. The intestine is obstructed at both ends, creating a “closed loop.”
A patient with an incomplete or partial small bowel obstruction (SBO) may be treated expectantly; however, if the obstruction is complete (distended small bowel and collapsed colon), and the patient complains of abdominal pain, intestinal viability is threatened. Hence the adage, “Never let the sun set on a patient with intestinal obstruction!”
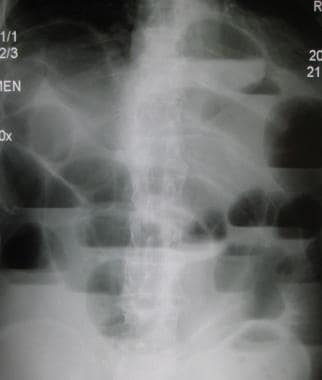
Intestinal obstruction in the newborn. Upright radiograph in a patient with complete intestinal obstruction. Note the air-fluid levels and absence of air in the colon.