
Practice Essentials
Conventional chest radiography is generally the first imaging procedure performed in patients with respiratory symptoms, and frontal and lateral chest radiographs may reveal changes of emphysema. A chest radiograph is universally available, noninvasive, and inexpensive, and it poses an acceptable radiation exposure.
Chest radiographic findings are not good indicators of the severity of disease and do not help in identifying patients with chronic obstructive pulmonary disease (COPD) without clinically significant emphysema.
High-resolution computed tomography (HRCT) scanning is more sensitive than chest radiography in diagnosing emphysema and in determining its type and extent of disease.
HRCT also has a high specificity for diagnosing emphysema with virtually no false-positive diagnoses, but in clinical practice, more reliance is placed on patient history, lung function tests, and abnormal chest radiographs to diagnose emphysema. However, some patients with early emphysema, particularly those with early disease, may present with atypical symptoms, and it is in these patients that an HRCT is most rewarding. If significant emphysema is found on HRCT, no further workup is necessary; specifically, lung biopsy is not needed. Imaging information from HRCT does not alter the management of emphysema; therefore, HRCT has no place in the day-to-day care of patients with COPD. In their early stages, the 3 forms of emphysema can be distinguished morphologically by using HRCT, but as the disease becomes more extensive, the distinction becomes difficult or impossible, both radiographically and pathologically.
A number of studes have assessed the role of computed tomography (CT) in the early detection of lung cancer in patients with COPD and in predicting response to lung-volume–reduction surgery (LVRS).
CT scans are used to characterize the emphysema and degree of destruction on a lobar basis, to evaluate the distribution of the emphysema destruction, and to determine the integrity of the lobar fissures.
CT characterization of heterogeneous parenchymal abnormalities can provide criteria for selection of the preferable treatment in each patient and improve the outcome of LVR. In particular, emphysema distribution pattern and fissures integrity can be evaluated to tailor the choice of the most appropriate LVR technique.
Radionuclide scanning and MRI may have a potential role in patients being assessed for LVRS.
(Images of emphysema are displayed below.)
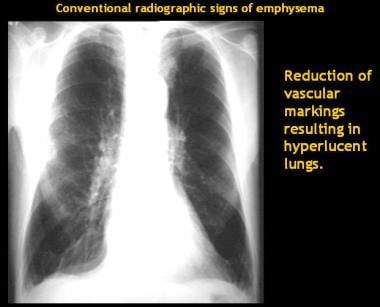
Chest radiograph of an emphysematous patient shows hyperinflated lungs with reduced vascular markings. Pulmonary hila are prominent, suggesting some degree of pulmonary hypertension (Corrêa da Silva, 2001).

CT densitovolumetry in a heavy smoker with emphysema revealed compromise of about 22% of the lung parenchyma (Corrêa da Silva, 2001).

CT densitovolumetry in a patient with lung cancer. Three-dimensional (3D) image shows that the cancer is in the portion of the right lung that was less affected by emphysema in a patient with poor pulmonary function (Corrêa da Silva, 2001).
Ballile and Laennec described the anatomopathology of emphysema in 1793 and in 1826, respectively. After that, Lynne Reid published one of the landmark works in our understanding of emphysema, The Pathology of Emphysema,
which provided a detailed description of the anatomy of the lung units and of the anatomopathology and pathophysiology of emphysema, broadening the view of this complex disease.
Pulmonary emphysema is defined as the permanent enlargement of airspaces distal to the terminal bronchioles and the destruction of the alveolar walls. Pathology reveals a marked increase in the size of the airspaces, resulting in labored breathing and an increased susceptibility to infection. It can be caused by irreversible expansion of the alveoli or by the destruction of alveolar walls. Fibrosis is not associated with this condition.
Pulmonary emphysema and chronic bronchitis are important components of chronic obstructive pulmonary disease. Emphysema often coexists with chronic bronchitis in the COPD population, and from a clinical point of view, they are generally considered as one entity. Although a tissue diagnosis of emphysema is possible, in advanced cases it can usually be confidently diagnosed on the basis of the patient’s history, physical findings, pulmonary function, and imaging results.
For further information, see Imaging in Congenital Lobar Emphysema, Imaging in Emphysematous Pyelonephritis, and Imaging in Pulmonary Interstitial Emphysema.