
Practice Essentials
Asthma is a common chronic disease worldwide and affects approximately 26 million persons in the United States. It is the most common chronic disease in childhood, affecting an estimated 7 million children. The pathophysiology of asthma is complex and involves airway inflammation, intermittent airflow obstruction, and bronchial hyperresponsiveness. See the image below.
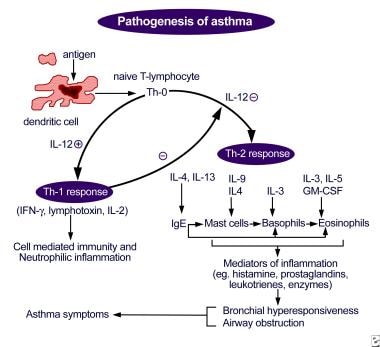
Pathogenesis of asthma. Antigen presentation by the dendritic cell with the lymphocyte and cytokine response leading to airway inflammation and asthma symptoms.
Signs and symptoms
Signs and symptoms of asthma include the following:
Wheezing
Coughing
Shortness of breath
Chest tightness/pain
Other nonspecific symptoms in infants or young children may be a history of recurrent bronchitis, bronchiolitis, or pneumonia; a persistent cough with colds; and/or recurrent croup or chest rattling.
See Clinical Presentation for more detail.
Diagnosis
Updated guidelines from the National Asthma Education and Prevention Program (NAEPP) highlight the importance of correctly diagnosing asthma, by establishing the following
:
Episodic symptoms of airflow obstruction are present
Airflow obstruction or symptoms are at least partially reversible
Exclusion of alternative diagnoses
Spirometry with postbronchodilator response should be obtained as the primary test to establish the asthma diagnosis. Pulse oximetry measurement is desirable in all patients with acute asthma to exclude hypoxemia. The chest radiograph remains the initial imaging evaluation in most individuals with symptoms of asthma, but in most patients with asthma, chest radiography findings are normal or may indicate hyperinflation. Exercise spirometry is the standard method for assessing patients with exercise-induced bronchoconstriction.
See Workup for more detail.
Management
For all but the most severely affected patients, the ultimate goal is to prevent symptoms, minimize morbidity from acute episodes, and prevent functional and psychological morbidity to provide a healthy (or near healthy) lifestyle appropriate to the age of child.
Pharmacologic treatment
Pharmacologic management includes the use of relief and control agents. Control agents include inhaled corticosteroids, long-acting bronchodilators (beta-agonists and anticholinergics), theophylline (Theo-24, Theochron, Uniphyl), leukotriene modifiers, anti-IgE antibodies, anti-interleukin (IL)–5 antibodies, and anti–IL-4/IL-13 antibodies. Relief medications include short-acting bronchodilators, systemic corticosteroids, and ipratropium (Atrovent).
The pharmacologic treatment of asthma is based on stepwise therapy. Asthma medications should be added or deleted as the frequency and severity of the patient’s symptoms change.
Allergen avoidance
Environmental exposures and irritants can play a strong role in symptom exacerbations. The use of skin testing or in vitro testing to assess sensitivity to perennial indoor allergens is important. Once the offending allergens are identified, counsel patients on how to avoid them. Efforts should focus on the home, where specific triggers include dust mites, animals, cockroaches, mold, and pollen.
See Treatment and Medication for more detail.