
Practice Essentials
Down syndrome is by far the most common and best known chromosomal disorder in humans and the most common cause of intellectual disability. It is primarily caused by trisomy of chromosome 21 (see the image below), which gives rise to multiple systemic complications as part of the syndrome. However, not all defects occur in each patient; there is a wide range of phenotypic variation.
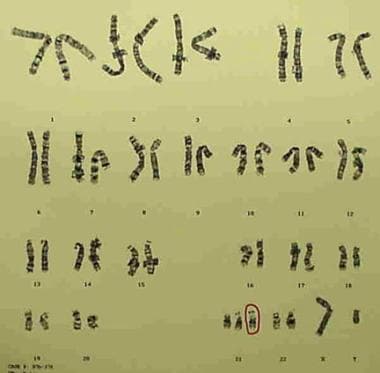
G-banded karyotype showing trisomy 21 (47,XY,+21).
Signs and symptoms of Down syndrome
When recording the history from the parents of a child with Down syndrome, the clinician should include the following:
Parental concern about hearing, vision, delay in growth and development, respiratory infections, and other problems
Feeding history to ensure adequate caloric intake
Prenatal diagnosis of Down syndrome
Vomiting secondary to gastrointestinal tract blockage by duodenal web or atresia
Absence of stools secondary to Hirschsprung disease
Delay in cognitive abilities, motor development, language development (specifically expressive skills), and social competence
Arrhythmia, fainting episodes, palpitations, or chest pain secondary to a heart lesion
Symptoms of sleep apnea, including snoring, restlessness during sleep, difficulty awaking, daytime somnolence, behavioral changes, and school problems
On physical examination, patients with trisomy 21 have characteristic craniofacial findings, such as the following:
Flat occiput and a flattened facial appearance
Small brachycephalic head
Epicanthal folds
Flat nasal bridge
Upward-slanting palpebral fissures
Brushfield spots
Small nose and small mouth
Protruding tongue
Low-set, small, and dysplastic ears
Short neck and generous nuchal skin
General physical features in patients with Down syndrome may include the following:
Shortened extremities
Short, broad hands, with short fifth finger with hypoplasia of the middle phalanx and clinodactyly, along with single transverse palmar creases (~60% of patients)
Joint hyperextensibility or hyperflexibility
Neuromuscular hypotonia
Diastasis recti
Dry skin
Premature aging
Congenital heart defects
Complications of Down syndrome can involve almost every organ system of the body.
See Presentation for more detail.
Diagnosis of Down syndrome
Laboratory studies that may be helpful include the following:
Complete blood count with differential
Bone marrow examination to rule out leukemia
Thyroid-stimulating hormone (TSH) and thyroxine (T4) to rule out hypothyroidism
Papanicolaou smears every 1-3 years in sexually active women
Cytogenetic studies (karyotyping) for diagnosis of trisomy 21
Interphase fluorescence in situ hybridization (FISH) for rapid diagnosis of trisomy 21
Assessment of mosaicism for trisomy 21 (lymphocyte preparations, buccal mucosa cellular preparations, FISH, scoring frequency of trisomic cells)
Immunoglobulin G
Maternal serum biochemical markers
Current evidence does not support performing routine screening radiographs for the assessment of potential atlantoaxial instability in asymptomatic children. However, imaging studies that may be considered include the following:
Echocardiography in every newborn suspected of having trisomy 21 to identify congenital heart disease, since approximately 50% of those with Down syndrome will have congenital heart disease
Ultrasonography
Postnatal diagnostic tests that may be warranted include the following:
Auditory brainstem response (ABR), or brainstem auditory evoked response (BAER)
Pediatric ophthalmic examination
See Workup for more detail.
Management
There are no medical treatments for intellectual disability associated with Down syndrome, but improved medical care has greatly enhanced quality of life and increased life expectancy. The American Academy of Pediatrics has issued guidelines for the care of children with Down syndrome.
Elements of medical care include the following:
Genetic counseling
Standard immunizations and well-child care
Management of specific manifestations of Down syndrome and associated conditions (eg, endocrine, infectious, cardiac, respiratory, neurologic, psychiatric, dermatologic, and dental disorders)
Early intervention programs (may improve the social quotient)
Special considerations in adolescents are as follows:
Ongoing monitoring measures, including annual audiologic evaluation and annual ophthalmologic evaluation
Ongoing management of manifestations of the syndrome and associated conditions
Discussion of issues related to the transition to adulthood
Vocational training
Appropriate surgical management of associated conditions should be provided, as follows:
Timely surgical treatment of cardiac anomalies is crucial for optimal survival
Prompt surgical repair is necessary for gastrointestinal (GI) anomalies, most commonly, duodenal atresia and Hirschsprung disease
Surgical intervention may be necessary to stabilize the upper segment of the cervical spine if neurologic deficits are clinically significant
Congenital cataracts must be extracted soon after birth and subsequent correction with glasses or contact lenses provided
Careful anesthetic airway management is needed because of the associated risk of cervical spine instability
Adenotonsillectomy may be performed to manage obstructive sleep apnea
See Treatment and Medication for more detail.