
Background
Sir William Osler was one of the first to recognize the bicuspid aortic valve as a common congenital anomaly of the heart.
Leonardo da Vinci recognized the superior engineering advantages of the normal trileaflet valve.
However, bicuspid aortic valve is mentioned only briefly in many pediatric and cardiology textbooks.
Definition
The normal aortic valve has 3 equal-sized leaflets or cusps with 3 lines of coaptation. A congenitally bicuspid aortic valve has 2 functional leaflets. Most have one complete line of coaptation. Approximately half of cases have a low raphe. Stenotic or partially fused valves caused by inflammatory processes, such as rheumatic fever, are not included.
Embryology
The embryonic truncus arteriosus is divided by the spiral conotruncal septum during development. The normal right and left aortic leaflets form at the junction of the ventricular and arterial ends of the conotruncal channel. The nonseptal leaflet (posterior) cusp normally forms from additional conotruncal channel tissue. Abnormalities in this area lead to the development of a bicuspid valve, often through incomplete separation (or fusion) of valve tissue.
Bicuspid aortic valve is often observed with other left-sided obstructive lesions such as coarctation of the aorta or interrupted aortic arch, suggesting a common developmental mechanism.
Specific gene mutations have been isolated.
Anatomy
The bicuspid valve is composed of 2 leaflets or cusps, usually of unequal size.
See the image below.
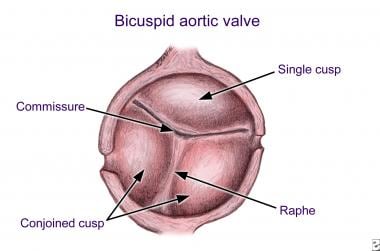
Bicuspid aortic valve with unequal cusp size. Note eccentric commissure and raphe.
The larger leaflet is referred to as the conjoined leaflet. Two commissures (or hinge points) are present; usually, neither is partially fused. The presence of a partially fused commissure, which has also been called a high raphe, probably predisposes toward eventual stenosis. At least half of all congenitally bicuspid valves have a low raphe, which never attains the plane of the attachments of the two commissures and never extends to the free margin of the conjoined cusp. Redundancy of a conjoined leaflet may lead to prolapse and insufficiency.
Valve leaflet orientation and morphology can vary. A recent surgical study showed conjoined leaflets in 76% of specimens.
Of these, fusion of the raphe was noted between the right and left cusps in 86%, and fusion was noted between the left and noncoronary cusps in only 3%. Of the valves without raphes, more than 30% of the leaflets were unequal in size.
Coronary arteries may be abnormal.
A left-dominant coronary system (ie, posterior-descending coronary artery arising from the left coronary artery) is more commonly observed with bicuspid aortic valve. Rarely, the left coronary artery may arise anomalously from the pulmonary artery. The left main coronary artery may be up to 50% shorter in patients with a bicuspid aortic valve. Occasionally, the coronary ostium may be congenitally stenotic in association with bicuspid aortic valve.
The aortic root may be dilated.
This dilatation has some similarities to the dilatation of the aorta seen in Marfan syndrome.
The dilatation may involve the ascending aorta (most commonly) but may also involve the aortic root or transverse aortic arch.
A recent study compared aortic dilation in children who had bicuspid aortic valve with and without coarctation of the aorta; the conclusion was that valve morphologic characteristics and function and age at the time of coarctation of the aorta repair had no impact to minimal impact on aortic dimensions.