
Practice Essentials
In 1979, McCabe first described a cohort of patients with idiopathic, rapidly progressive bilateral sensorineural hearing loss (SNHL). These patients’ hearing improved after treatment with corticosteroids, thereby suggesting an autoimmune pathogenesis. The hallmark of this clinically diagnosed condition is the presence of a rapidly progressive, often fluctuating, bilateral SNHL over a period of weeks to months. The progression of hearing loss is too rapid to be diagnostic for presbycusis and too slow to conclude a diagnosis of sudden SNHL. Vestibular symptoms, such as true vertigo, generalized imbalance, and ataxia, may be present.
See the image below.
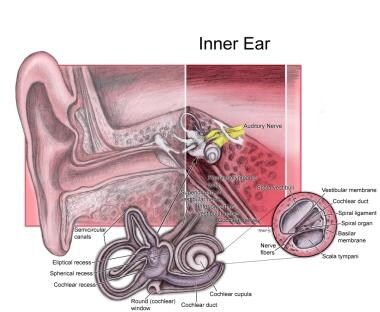
Inner ear.
Antigen-nonspecific tests are useful in routine screening for evidence of systemic immunologic dysfunction, yet specifically are not known to correlate with a diagnosis of immune-mediated inner ear disease.
Antigen-specific tests are as follows:
Migration inhibition assay
Lymphocyte transformation test (LTT)
Western blot analysis for antibodies to inner ear antigen
The natural history of untreated immune-mediated inner ear disease is unknown; much of the current therapy is based on empiric clinical data gathered during the past few decades. A key feature of immune-mediated inner ear disease is a positive response to immunosuppressive therapy (ie, corticosteroids) in the form of improved hearing.
Surgery generally is not appropriate for immune-mediated inner ear disease. However, intratympanic therapy performed under local anesthesia has been found to be beneficial for some patients.