
Practice Essentials
Malignant external otitis (MEO) is an infection that affects the external auditory canal and temporal bone. The causative organism is usually Pseudomonas aeruginosa, and the disease commonly manifests in elderly patients with diabetes. The infection begins as an external otitis that progresses into an osteomyelitis of the temporal bone. Spread of the disease outside the external auditory canal occurs through the fissures of Santorini and the osseocartilaginous junction.
Toulmouche was probably the first physician to report a case of malignant external otitis (MEO), in 1838. In 1959, Meltzer reported a case of pseudomonal osteomyelitis of the temporal bone. In 1968, Chandler discussed the clinical characteristics of malignant external otitis (MEO) and defined it as a distinct clinical disease.
He described this external otitis as malignant because he observed an aggressive clinical behavior, poor treatment outcome, and a high mortality rate for the patients affected by this disease.
The subsequent development of effective antibiotics for treating pseudomonal infections has improved the treatment outcomes for patients with malignant external otitis (MEO). Thus, some physicians have suggested that the term malignant should be abandoned in order to provide a more accurate description of the disease process.
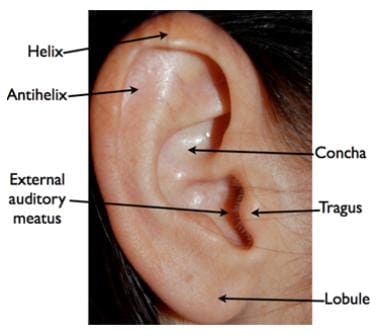
Anatomy of the ear.
Signs and symptoms of malignant otitis externa
Inflammatory changes are observed in the external auditory canal and the periauricular soft tissue.
The pain is out of proportion to the physical examination findings. Marked tenderness is present in the soft tissue between the mandibular ramus and mastoid tip. Granulation tissue is present at the floor of the osseocartilaginous junction. This finding is virtually pathognomonic of malignant external otitis (MEO). Otoscopic examination may also reveal exposed bone.
Other signs and symptoms include the following:
Diabetes (90%) or immunosuppression (illness or treatment related)
Severe, unrelenting, deep-seated otalgia
Temporal headaches
Purulent otorrhea
Possibly dysphagia, hoarseness, and/or facial nerve dysfunction
Diagnosis and management of malignant otitis externa
The leukocyte count in malignant external otitis (MEO) is usually normal or mildly elevated. A left shift is not commonly found. The erythrocyte sedimentation rate (ESR) is invariably elevated, with an average of 87 mm/h.
Patients with known diabetes need an evaluation of the serum chemistry to determine if the infection is affecting their baseline glucose intolerance. Patients without a history of diabetes should be tested for glucose intolerance.
Culture from the ear drainage should be performed ideally before antimicrobial therapy is initiated. As mentioned, the most common causative organism is P aeruginosa (95%).
Imaging studies are important for determining the presence of osteomyelitis, the extent of disease, and response to therapy. They include technetium Tc 99 methylene diphosphonate bone scanning, gallium citrate Ga 67 scanning, indium In 111–labeled leukocyte scanning, computed tomography (CT) scanning, and magnetic resonance imaging (MRI).
Obtain a biopsy of the external auditory canal to exclude carcinoma or other etiologies.
Treatment for malignant external otitis (MEO) includes meticulous glucose control, aural toilet, systemic and ototopic antimicrobial therapy, and hyperbaric oxygen therapy.
Surgery is now reserved for local debridement, removal of bony sequestrum, and abscess drainage.