
Practice Essentials
Atherosclerosis is a diffuse, degenerative disease of the arteries that results in the formation of plaques composed of necrotic cells, lipids, and cholesterol crystals. These plaques can cause stenosis (see the image below), embolization, and thrombosis. Atherosclerosis has a predilection for certain arteries, including the extracranial carotid artery.
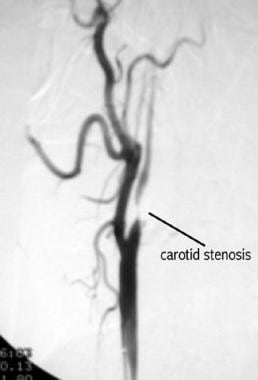
Arteriogram of carotid stenosis.
Signs and symptoms
Atherosclerotic disease of the carotid artery may be associated with the following:
Amaurosis fugax (transient ipsilateral visual loss)
Transient ischemic attacks (TIAs)
Crescendo TIAs
Stroke-in-evolution
Cerebral infarction
See Overview for more detail.
Indications and contraindications for carotid endarterectomy
Indications
Indications for carotid endarterectomy (CEA), based on prospective randomized trials, include the following:
Symptomatic patients with greater than 70% stenosis – Clear benefit was found in the North American Symptomatic Carotid Endarterectomy Trial (NASCET)
Symptomatic patients with greater than 50-69% stenosis – Benefit is marginal; appears to be greater for male patients
Asymptomatic patients with greater than 60% stenosis – Benefit is significantly less than for symptomatic patients with greater than 70% stenosis
Note: The percentage of stenosis used as the threshold for CEA varies among available literature. Generally, symptomatic patients with greater than 50% stenosis and healthy, asymptomatic patients with greater than 60% stenosis warrant consideration for CEA.
Contraindications
Contraindications for CEA include the following:
Patients with a severe neurologic deficit following a cerebral infarction
Patients with an occluded carotid artery
Concurrent medical illness that would significantly limit the patient’s life expectancy
Laboratory and radiologic studies
Studies to be considered include the following:
Complete blood count
Levels of electrolytes, blood urea nitrogen, creatinine
Lipid profile
Coagulation studies – Prothrombin time/activated partial thromboplastin time
Electrocardiography – To identify evidence of prior MI as well as ischemic changes
Carotid duplex ultrasonography, with or without color – Screening test of choice to evaluate for carotid stenosis
Cranial computed tomography or magnetic resonance imaging – To rule out other intracranial lesions and to identify the presence of new and old cerebral infarcts
Carotid magnetic resonance angiography – May be useful in collaborating the finding of an occluded carotid with duplex sonography; however, this modality tends to overstate the significance of the stenosis
Aortic arch and carotid arteriography – To evaluate the percentage of stenosis
See Workup for more detail.
Management
Treatment of atherosclerosis of the carotid artery is dependent on the severity and degree of the disease.
Pharmacotherapy
Medications used to manage atherosclerotic disease of the carotid artery include the following:
Antiplatelet agents (eg, aspirin, ticlopidine, clopidogrel)
Statin therapy (atorvastatin, rosuvastatin, simvastatin, pravastatin, lovastatin)
Anticoagulants (eg, warfarin) – Note that the use of warfarin in patients with noncardiac emboli is controversial
Surgery
Endovascular management of atherosclerotic disease of the carotid artery includes the following procedures:
CEA
Carotid angioplasty and stenting (CAS)
Transcarotid artery revascularization (TCAR)
See Treatment for more detail.