
Practice Essentials
Erectile dysfunction (ED), formerly termed impotence, is defined as “the inability to attain and/or maintain penile erection sufficient for satisfactory sexual performance” or “the consistent or recurrent inability to attain and/or maintain penile erection sufficient for sexual satisfaction”.
Although some cases, particularly in younger men, may primarily reflect psychological concerns, in many cases ED results from organic disease—notably, cardiovascular disease, diabetes mellitus, hyperlipidemia, and hypertension.
Thus, ED may serve as a marker for medical conditions in need of treatment.
Regardless of the cause, however, ED can have negative effects on patients’ self-esteem, relationships, and overall quality of life.
Signs and symptoms
The first step in the management of ED is a thorough history that includes the following:
Sexual history
Medical history
Psychosocial history
A physical examination is necessary for every patient, emphasizing the genitourinary, vascular, and neurologic systems. A focused examination entails evaluation of the following:
Blood pressure
Peripheral pulses
Sensation
Status of the genitalia and prostate
Size and texture of the testes
Presence of the epididymis and vas deferens
Abnormalities of the penis (eg, hypospadias, Peyronie plaques)
There is a strong correlation between hypertension and ED. There is also a correlation between benign prostatic hyperplasia and ED, though the causality is unclear.
See Presentation for more detail.
Diagnosis
Laboratory testing for ED depends on information gathered during the interview; it is necessary for most patients, although not for all. Such testing may include the following:
Evaluation of hormonal status (testosterone, serum hormone–binding globulin, luteinizing hormone [LH], prolactin, thyroid-stimulating hormone [TSH]) – Note that the American College of Physicians (ACP) does not recommend for or against routine use of hormonal blood tests or hormonal treatment in ED patients
Screening blood studies (hemoglobin A1c, serum chemistry panel, lipid profile)
Prostate-specific antigen levels, if the patient is a candidate for prostate cancer screening (controversial)
Urinalysis
Functional tests that may be helpful include the following:
Direct injection of prostaglandin E1 (PGE1; alprostadil) into the corpora cavernosa (see the image below)
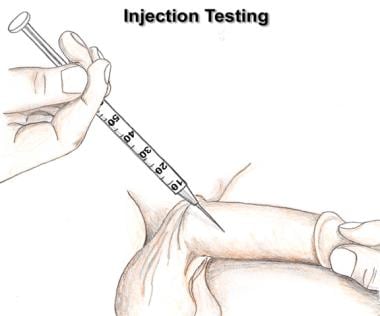
A vasodilator such as prostaglandin E1 can be injected into one of the corpora cavernosa. If the blood vessels are capable of dilating, a strong erection should develop within 5 minutes.
Biothesiometry – Infrequently indicated
Nocturnal penile tumescence testing – Once frequently performed, this is rarely used in current practice, though it can be helpful when the diagnosis is in doubt
Formal neurologic testing – Not needed in the vast majority of ED patients, though it may offer some benefit to patients with a history of central nervous system problems, peripheral neuropathy, diabetes, or penile sensory deficit
Imaging studies are not commonly warranted, except in situations where pelvic trauma has been sustained or surgery performed. Modalities that may be considered include the following:
Ultrasonography of the penis (to assess vascular function within the penis)
Ultrasonography of the testes (to help disclose abnormalities in the testes and epididymides; rarely indicated)
Transrectal ultrasonography (to disclose abnormalities in the prostate and pelvis that may interfere with erectile function)
Angiography (in patients who are potential candidates for vascular surgery)
See Workup for more detail.
Management
Treatment options for ED include the following:
Sexual counseling, if no organic causes can be found for the dysfunction
Oral medications
Injected, implanted, or topically applied medications
External vacuum and constriction devices
Surgery
Many patients with ED also have cardiovascular disease; thus, treatment of ED in these patients must take cardiovascular risks into account.
According to American Urological Association (AUA) guidelines, oral phosphodiesterase type 5 (PDE5) inhibitors are first-line therapy unless contraindicated.
Agents include the following:
Sildenafil
Vardenafil
Tadalafil
Avanafil
In patients with ED refractory to oral PDE5 inhibitors, one of these agents can be combined with an injection of PGE1.
In a prospective, multicenter, single-armed study of ED patients who exhibited a suboptimal response to PDE5 inhibitors, the investigators found that percutaneous implantation of zotarolimus-eluting stents in focal atherosclerotic lesions was both safe and feasible and was associated with clinically meaningful improvement on subjective and objective measures of erectile function.
Hormone replacement may benefit men with severe hypogonadism and may possibly be useful as adjunctive therapy when other treatments are unsuccessful. Replacement androgens are available in oral (rarely used), injectable, gel, and transdermal preparations.
Intracavernosal injection therapy may be considered and is almost always effective if the vasculature within the corpora cavernosa is healthy. Agents used include the following:
Alprostadil (most common)
Phentolamine
Papaverine
The Medicated Urethral System for Erections (MUSE) involves the formulation of alprostadil (PGE1) into a small intraurethral suppository that can be inserted into the urethra. This may be useful for men who do not want to use self-injections or those in whom oral medications have failed.
External devices that may be used include the following:
Vacuum devices to draw blood into the penis
Constriction devices placed at the base of the penis to maintain erection
Selected patients with ED are candidates for surgical treatment. Procedures to be considered include the following:
Revascularization (rarely indicated)
Surgical elimination of venous outflow (rarely indicated)
Placement of penile implant (semirigid or malleable rod implant, fully inflatable implant, or self-contained inflatable unitary implant) – Once the only effective therapy for men with organic ED, this is the last option considered in current practice
Suggested measures for preventing ED include the following:
Optimal management of diabetes, heart disease, and hypertension
Lifestyle modifications to improve vascular function (eg, not smoking, maintaining ideal body weight, and engaging in regular exercise)
See Treatment and Medication for more detail.