
Practice Essentials
Shoulder pain is the third most common reason for musculoskeletal consultations in the primary care setting, affecting up to one third of the general population.
Of patients presenting with shoulder symptoms, 80% remain symptomatic 6 months later, and 50% have symptoms at 18 months. Shoulder pain is usually poorly localized, with the exception of pain occurring in the acromioclavicular joint.
In patients older than 40 years, the main causes of shoulder pain and/or functional deficit are adhesive capsulitis (frozen shoulder) and impingement and/or rotator cuff disease. Ultrasonography has a proven role in assessing tendons of the rotator cuff.
This examination is used to identify and classify pathology, and it can help clinicians in making decisions about ongoing management of the condition.
The advantages of US include low cost, accessibility, and capability for real-time high-resolution imaging that enables dynamic assessment and needle guidance. The additional benefits of US, as compared with MRI, include patient satisfaction; the opportunity for patient-clinician interaction and real-time feedback; the lack of contraindications such as pacemakers, which preclude the use of MR imaging; the capability for evaluation in the setting of artifact-prone surgical hardware; and the capability for comparison with findings in the contralateral anatomy.
(Ultrasonograms of rotator cuff injuries are shown below.)
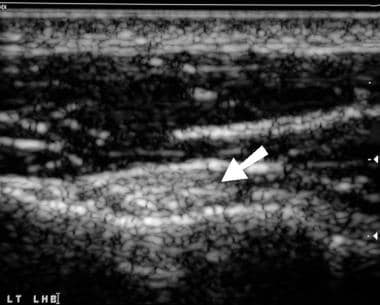
Shoulder, rotator cuff injury (ultrasonography). Ultrasonographic view transverse to the long head of biceps tendon (arrow).
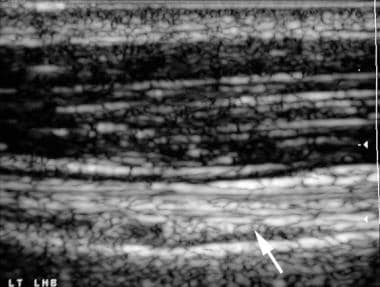
Shoulder, rotator cuff injury (ultrasonography). Ultrasonographic view longitudinal to the long head of biceps tendon (arrow).
Preferred examination
Radiographic evaluation is generally the first imaging study ordered in patients with shoulder pain. According to the American College of Radiology (ACR) Appropriateness Criteria, in certain instances where clinical examination suggests rotator cuff disease or adhesive capsulitis, symptoms of impingement, or painful palpable mass, sonography may be considered as an initial imaging study.
Good-quality ultrasound equipment is essential to produce satisfactory images of the cuff tendons with good resolution. A high frequency (7- to 15-MHz) linear-array probe is required.
Examination techniques vary, with some operators preferring to face the patient and others preferring to stand behind the patient, scanning over the patient’s shoulder.
The long head of the biceps tendon is examined within the intertubercular groove, in both the transverse and longitudinal planes, with the patient’s arm in a neutral position and the elbow flexed to 90° (see the first 2 images below). The presence of fluid around the tendon is noted (see the third image below), and a search for fluid in the subdeltoid bursa is made. With the shoulder externally rotated, the subscapularis tendon is brought into view and examined in both planes, with the imager taking care not to misinterpret the multipennate nature of the tendon as an indication of a tear. A search for subluxation or dislocation of the long head of the biceps tendon is made at this stage.
Shoulder, rotator cuff injury (ultrasonography). Ultrasonographic view transverse to the long head of biceps tendon (arrow).
Shoulder, rotator cuff injury (ultrasonography). Ultrasonographic view longitudinal to the long head of biceps tendon (arrow).
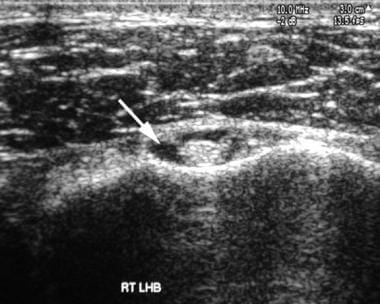
Shoulder, rotator cuff injury (ultrasonography). Ultrasonographic view transverse to the long head of biceps tendon, which is surrounded by nonechogenic fluid (arrow).
Then, the patient is asked to rotate the shoulder internally. This movement is achieved either by placing the forearm behind the back with the palm facing posteriorly or by placing the palm on the upper buttock. Both positions provide slightly different degrees of internal rotation and may be used in combination. The supraspinatus and infraspinatus tendons are now evaluated (as shown in the images below) in both the transverse and longitudinal planes. The presence of fluid in the bursa may be assessed again, as may the contour of the bony surface of the humerus. The examination is completed by requesting the patient to place a hand on the contralateral shoulder. This position allows further assessment of the infraspinatus tendon if required, providing a view of the acromioclavicular joint under stress and a deep view of the spinoglenoid notch where ganglia or other mass lesions can cause compression of the suprascapular nerve.
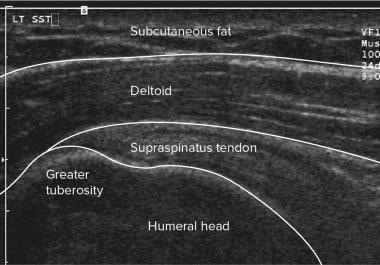
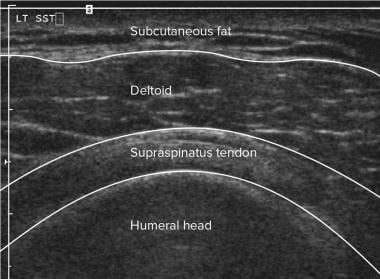
Shoulder, rotator cuff injury (ultrasonography). Diagrammatic longitudinal view of the supraspinatus tendon.
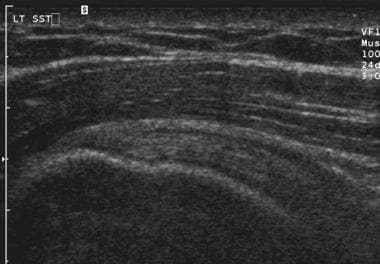
Shoulder, rotator cuff injury (ultrasonography). Longitudinal ultrasonographic view of the normal supraspinatus tendon (compare with the previous image).
Shoulder, rotator cuff injury (ultrasonography). Diagrammatic transverse view of the supraspinatus tendon.
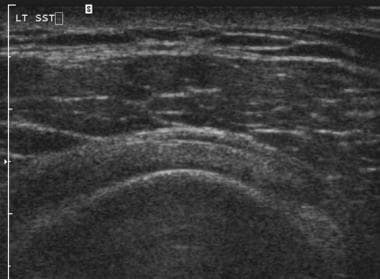
Shoulder, rotator cuff injury (ultrasonography). Transverse ultrasonographic view of the normal supraspinatus tendon (compare with the previous image).
Dynamic evaluation of abduction can be performed by observing the supraspinatus tendon and bursa longitudinally as they retract deep to the coracoacromial ligament. Bunching of tissue or buckling of the ligament correlates with impingement.
Limitations of techniques
Successful use of ultrasound to examine the shoulder depends on the operator, machine, and patient factors. Knowledge of the relevant anatomy and pathologic appearances and experience in performing the technique are required of operators. Machine requirements are discussed above in Preferred Examination.
Ultrasonography is comparable to MRI in evaluating full-thickness rotator cuff tears and rotator cuff atrophy; however, it is inferior to MRI in evaluating partial-thickness rotator cuff tears and other intra-articular pathology.
As in other regions of the body, ultrasonography of the shoulder is limited in obese patients, and views of the tendons are restricted in patients with severely limited range of movement. Ultrasonography cannot be used to directly image the subacromial space, and it provides no information about the inferior surface of the acromioclavicular joint. Ultrasonography can show the contour of bony surfaces, but no information can be obtained beneath the surface. The subacromial space is not accessible, and pathology, including the retracted end of a torn tendon, cannot be shown in this location.
Operators should be familiar with the effects of anisotropy, an artifact found on sonograms of tendons. Tendons consist of parallel collagen bundles that reflect transmitted sound. If the probe is not held with the surface parallel to the tendon, reflection is not back toward the probe, and the tendon may falsely appear hyporeflective. In other words, anisotropy occurs when the footprint of the ultrasound transducer is not parallel to the tendon and the ultrasound beam is not perpendicular to the long axis of the tendon. The resulting appearance may simulate that of disease (compare the images below).
Shoulder, rotator cuff injury (ultrasonography). Ultrasonographic view transverse to the long head of biceps tendon (arrow).
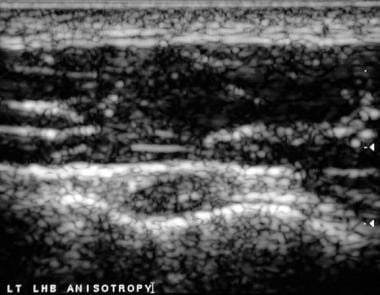
Shoulder, rotator cuff injury (ultrasonography). Transverse ultrasonographic view of the long head of biceps tendon with probe angulation. The alteration in probe angle causes the ultrasound beam to intersect the tendon at an angle other than 90° and causes reduced reflectivity within the tendon resulting from anisotropic artifact.
For MRI findings, see Shoulder, Rotator Cuff Injury (MRI).
Intervention
Ultrasonography can easily be used to guide accurate needle placement for an injection of a local anesthetic or a corticosteroid into the subdeltoid bursa. This injection can be used to confirm impingement and to treat symptoms. If bubbles of gas subsequently are found within the glenohumeral joint, the presence of a full-thickness tear can be confirmed.
It also can be used to provide guidance for therapeutic intervention. US-guided barbotage has been shown to be a highly effective percutaneous treatment in patients with suspected calcific tendinitis.
In addition, US is the method of choice for newer methods of intratendinous therapy, including tenotomy, platelet-rich plasma (PRP), or autologous blood injections.
Patient education
For patient education information, see the Breaks, Fractures, and Dislocations Center, as well as Shoulder Dislocation and Shoulder Separation.