
Overview
Fractures of the thoracic spine may be seen in patients of any age, but in elderly patients, the frequency and severity of thoracic spinal fractures is increased. Fractures of the thoracic spine can occur whenever the spinal column is subjected to forces that exceed its strength and stability. Common causes of thoracic spinal fractures include falling from a height, motor vehicle accidents, violent weather, military and civilian blast injury, and penetrating trauma. Less common injury patterns may be related to sports injuries. The older patient presents an increased challenge because thoracic spinal fractures may occur following relatively minor falls. After aortic rupture, severe thoracic spinal cord injuries represent the most serious long-term morbidities resulting from thoracic trauma.
See the images below.

Thoracic spine trauma. Anterior view of multiple spinal cord contusions caused by burst compression fractures of the middle and lower thoracic spine.
The goals of diagnostic imaging in patients who have sustained thoracic spinal trauma are to correctly identify spinal fractures, to identify associated injuries to structures that are related to the thoracic spine, to identify injuries to the spinal cord and nerve roots, to aid in surgical planning, and to judge the stability of postoperative fixation.
In cases of multiple system trauma thoracic spinal fractures may be first discovered during the performance of CT of the chest and abdomen. Some authors have advocated a careful review of the axial CT images obtained in the typical CT trauma series without the additional use of thin section reformatted images.
In a study by Gross, the reformatting of chest CT scans and abdominopelvic CT scans were shown to provide improved sensitivity in detecting thoracic and lumbar spine fractures. There were 176 abdominopelvic CT scans with reformatting and 175 chest CT scans with reformatting. In the study, there were 9 of 176 false-negative abdominopelvic CT scans, versus 3 of 176 false-negative lumbar spine CT scans, and there were 14 of 175 false-negative chest CT scans, versus 2 of 175 false-negative thoracic spine CT scans. According to the authors, the differences in sensitivity were significant for both comparisons.
Pathophysiology
Compression fractures of the thoracic spine occur when a vertical force with or without a flexion or rotational sheer force exceeds the weight-bearing strength of the vertebral body. Various diseases, advanced age, and other comorbidities may make compression fractures more likely.
Fractures associated with subluxation or dislocation are more commonly the result of high-velocity blunt trauma with an element of flexion or rotational stress. In cases associated with unusual causes of spinal injury, such as child abuse, the mechanism of injury may be a complex combination of traumas to the thoracic spine. A high index of suspicion of abuse can help identify occult spinal fractures in younger patients.
In patients with ankylosing spondylitis, the incidence of thoracic spinal fractures is increased but the patterns of spinal fracture are unusual. Fractures in patients with ankylosis spondylitis are most commonly linear and horizontal in orientation.
Multiple myeloma commonly involves the thoracic spine, and fractures are more common. The surgical repair of fractures of the thoracic spine in patients with multiple myeloma is complicated by the multicentric nature of the disease.
Epidemiology
Thoracic spinal fractures remain a common component of trauma in the United States and in other developed nations with high rates of motor vehicle accidents.
Mortality due to motor vehicle traffic accidents declined in the United States during 2000-2009,
primarily because of better traffic conditions and improved emergency trauma services. During that same period, the number of deaths due to falls from a height increased.
Mechanical CPR devices have been identified as an unusual cause of thoracic spinal fractures.
The incidence of pathologic fractures due to osteoporosis is somewhat lower in black women than in persons of other races and greater in elderly women
Mortality/morbidity
Mortality of thoracic spinal fractures is most commonly related to injuries associated with aortic tear or rupture and cardiac trauma. Short-term morbidity is complicated by pulmonary disease and shock. Long-term morbidity among spinal fracture patients includes paralysis, sepsis, and the need for spinal stabilization. The means of aortic repair may include endovascular repair versus open surgical graft placement. The timing and nature of spinal fracture fixation is subject to regional and individual opinion.
The timing of surgical repair of a thoracic spinal fracture may make a difference in clinical outcome.
Anatomy
There are 12 thoracic vertebral bodies in the majority of people. The typical thoracic vertebral segment consists of a thoracic vertebral body, right and left transverse processes, a single posterior spinous process, and a right and left superior and inferior facet surface linked to the vertebral body by a pedicle. Each of the thoracic vertebral bodies is linked by the anterior longitudinal ligament, the posterior longitudinal ligament, the ligament flava, and the interspinal ligaments. The typical thoracic vertebral body has facet surfaces for the articulation of a right and left rib. The intervertebral distances between the thoracic vertebral bodies are less than the lumbar segments.
A thoracic nerve named for the vertebral segment exits laterally at the same numbered level. Each thoracic nerve root is formed from a ventral and a dorsal nerve root. A dorsal root ganglion is located inferior to the vertebral pedicle of the same number.
While most people have 12 ribs, the 12th rib may be rudimentary. Each rib is attached to the vertebral body by 2 joint cavities. The lateral costotransverse ligament, the articular capsule, the superior costotransverse ligament, and the intra-articular ligament provide flexible stability between the transverse process and the rib facets.
Depictions of the anatomy of the thoracic spine and vertebra are provided in the images below.
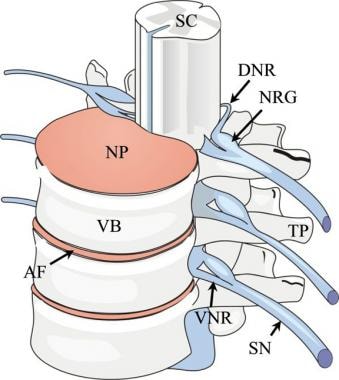
Thoracic spine trauma. Drawing of the thoracolumbar spine viewed from an oblique frontal projection. SC indicates the spinal cord; NP, nucleus pulposus; VB, vertebral body; AF, annulus fibrosis; VNR, ventral nerve root; SN, spinal nerve; TP, transverse process; DNR, dorsal nerve root; and NRG, nerve root ganglion.
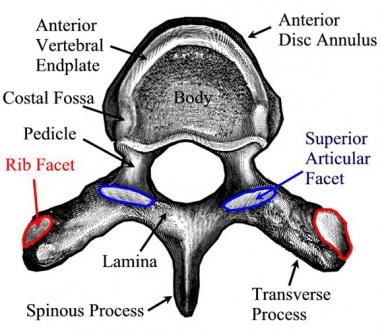
Thoracic spine trauma. Axial drawing of a typical thoracic vertebral body viewed from above. The thoracic vertebral bodies are unique in that ribs articulate by rib facets (red outline and red arrow) with the correspondingly numbered vertebrae. The superior articular facet (outlined in blue, blue arrow) is oriented along a lateral plane.
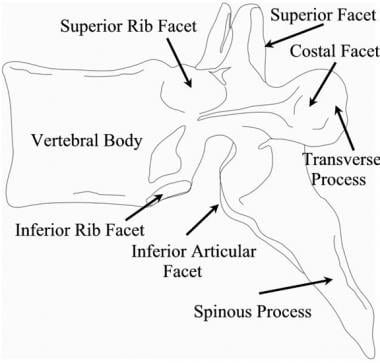
Thoracic spine trauma. Drawing of a typical thoracic vertebral body viewed in a lateral projection. The superior rib facet, semilunar inferior rib facet and the costal facet provide articulation for the ribs. The articular facet surfaces are oriented laterally. The spinous processes of the upper and mid thoracic vertebrae are angulated caudally.
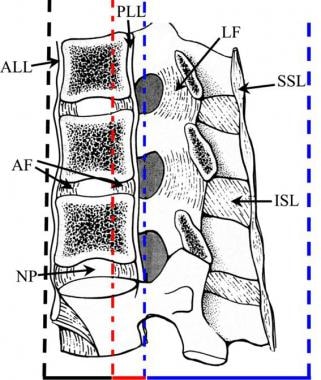
Thoracic spine trauma. Sagittal drawing of the thoracic spine demonstrating the structures that comprise the anterior, middle, and posterior columns. ALL indicates the anterior longitudinal ligament; AF, annulus fibrosus; NP, nucleus pulposus; PLL, posterior longitudinal ligament; SSL, supraspinous ligament; LF, ligamentum flavum; and ISL, interspinous ligament. Lateral drawing of the 3 spinal columns of the thoracolumbar junction. The anterior column is indicated by the black dotted line and includes the anterior spinal ligament, the anterior annulus fibrosis and the intervertebral disk, and the anterior two thirds of the vertebral bodies. The middle column (red dotted line) includes the posterior aspect of the vertebral bodies, the posterior annulus fibrosis, and the posterior longitudinal ligament. The posterior column (blue dotted line) includes all of the spine posterior to the longitudinal ligament (thick blue dotted line).

Thoracic spine trauma. Twelve similar thoracic vertebral bodies form the thoracic spine. A rib is attached to each of the vertebral bodies of the same number. The mild kyphosis of the thoracic spine occurs due to the slightly wedged shape of the anterior thoracic vertebral bodies.
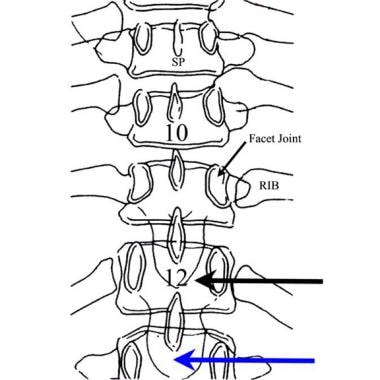
Thoracic spine trauma. Posterior drawing of the lower thoracic spine. The last rib usually is attached to the 12th thoracic vertebral body. Each thoracic vertebral body articulates with a rib. The facet joints of the thoracic region are oriented in an anterior to posterior direction. The first lumbar vertebral body (blue arrow) is similar to the last thoracic vertebral body (black arrow) except for the absence of a rib at T12.

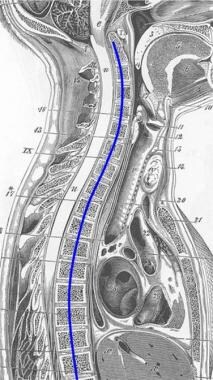
Thoracic spine trauma. Lateral drawing the spine with the natural spinal curves shown by a curved line. A normal lordotic curve of the cervical spine, a mild kyphosis of the thoracic spine, and lordosis of the lumbar region are noted. These curves act to distribute the vertical weight-bearing load most efficiently.
Thoracic spine trauma. The natural lordotic curvature of the cervical spine is reversed in the upper thoracic spine to form a kyphosis in the T1-T2-T3 segments in most adults.
In general, anteroposterior (AP) and lateral radiographs should be obtained in the emergency department while other measures of resuscitation are performed. Multidetector CT scans with intravenous contrast enhancement are indicated in most patients to exclude intrathoracic vascular injury. In patients who have sustained blunt trauma, multidetector CT has been proposed as a screening study for thoracolumbar fracture.
MRI of the thoracic spine should be reserved for patients with neurologic deficits or patients with spinal canal compromise who are unable to provide a full neurologic history. MRI of the thoracic region provides important information concerning the spinal cord and the dural structures.
Note the images below.
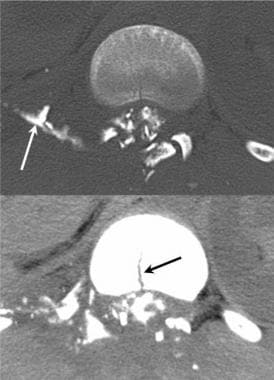
Thoracic spine trauma. Axial CT myelogram in a patient with a gunshot wound to the thoracic spine. While a fracture is obvious, the injury also resulted in a dural tear with a freely leaking cerebrospinal fluid space (white arrow). The midline fracture of the vertebral body is noted in the lower image (black arrow).
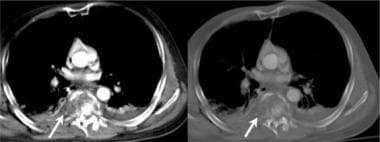
Thoracic spine trauma. Axial CT image demonstrates a complex fracture of the T12 with rotation subluxation. Air was introduced into the epidural space during the injury.
Patients with osteoporotic vertebral fractures may require a comprehensive approach to spinal imaging.
Many patients who present with thoracic injury have a pulmonary, rib, or vascular injury. Most patients who have sustained multiple system trauma will have had a CT of the chest and abdomen as part of their evaluation. Pregnant women should be imaged carefully while limiting radiation exposure if possible.
The expense and delay of obtaining routine CT scans of the thoracic spine are not justified in all cases. Focused CT scans should be performed if patients have unexplained thoracic back pain or neurological symptoms.
A review of the bone windows of thoracic CT scans indicates most major deformities associated with Chance fracture, distraction injury, and burst vertebral fractures. The more complex injuries can be studied later if necessary. Multisectional axial CT of the thoracic region should be reformatted to examine the thoracic spine in a lateral (sagittal) view.
The application of MRI in spinal trauma should be linked to an abnormality of the neurologic examination or to an evaluation of unexplained severe spinal pain.
Clinical details
The Denis classification is considered clinically useful in the description of spinal fractures. Although the Denis classification provides a useful framework for describing the initial bony injury and the neurologic deficits, neurological recovery has been reported to have a poor correlation.
Differentials
Thoracic Discogenic Pain Syndrome
Other problems to be considered
The initial evaluation of a patient with a thoracic spinal fracture should account for a possible multisystem trauma pattern (polytrauma). In such cases, possible cranial, abdominal, pelvic, and extremity injuries must be managed. The challenge for the radiologist in polytrauma is to effectively manage the large amount of information obtained by multiple radiographs, CT studies, and MRI scans.
Intervention
Open stabilization remains the most common surgical intervention for the treatment of unstable fractures and dislocations of the thoracic spine. Neurological symptoms and pain remain possible outcomes following open fixation with pedicle screws and rods. Osteoporotic and some pathological fractures can be stabilized with significant pain relief by the performance of a vertebroplasty or a kyphoplasty.
The recognition of the potential anomalous lower than ordinary position of the conus medullaris represents an important potential source of iatrogenic injury during the performance of spinal procedures, including myelography.