
Practice Essentials
Women with polycystic ovarian syndrome (PCOS) have abnormalities in the metabolism of androgens and estrogen and in the control of androgen production. PCOS can result from abnormal function of the hypothalamic-pituitary-ovarian (HPO) axis. A woman is diagnosed with polycystic ovaries (as opposed to PCOS) if she has 20 or more follicles in at least 1 ovary
(see the image below).
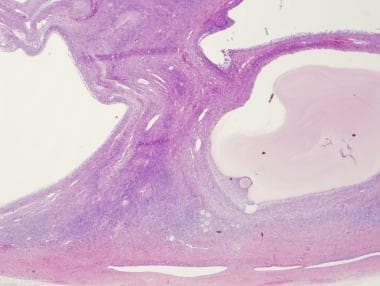
Low power, H and E of an ovary containing multiple cystic follicles in a patient with PCOS.
Signs and symptoms
The major features of PCOS include menstrual dysfunction, anovulation, and signs of hyperandrogenism.
Other signs and symptoms of PCOS may include the following:
Hirsutism
Infertility
Obesity and metabolic syndrome
Diabetes
Obstructive sleep apnea
See Clinical Presentation for more detail.
Diagnosis
On examination, findings in women with PCOS may include the following:
Virilizing signs
Acanthosis nigricans
Hypertension
Enlarged ovaries: May or may not be present; evaluate for an ovarian mass
Testing
Exclude all other disorders that can result in menstrual irregularity and hyperandrogenism, including adrenal or ovarian tumors, thyroid dysfunction, congenital adrenal hyperplasia, hyperprolactinemia, acromegaly, and Cushing syndrome.
Baseline screening laboratory studies for women suspected of having PCOS may include the following:
Thyroid function tests
(eg, TSH, free thyroxine)
Serum prolactin level
Total and free testosterone levels
Free androgen index
Serum hCG level
Cosyntropin stimulation test
Serum 17-hydroxyprogesterone (17-OHPG) level
Urinary free cortisol (UFC) and creatinine levels
Low-dose dexamethasone suppression test
Serum insulin-like growth factor (IGF)–1 level
Other tests used in the evaluation of PCOS include the following:
Androstenedione level
FSH and LH levels
GnRH stimulation testing
Glucose level
Insulin level
Lipid panel
Imaging tests
The following imaging studies may be used in the evaluation of PCOS:
Ovarian ultrasonography, preferably using transvaginal approach
Pelvic CT scan or MRI to visualize the adrenals and ovaries
Procedures
An ovarian biopsy may be performed for histologic confirmation of PCOS; however, ultrasonographic diagnosis of PCOS has generally superseded histopathologic diagnosis. An endometrial biopsy may be obtained to evaluate for endometrial disease, such as malignancy.
See Workup for more detail.
Management
Lifestyle modifications are considered first-line treatment for women with PCOS. Such changes include the following
:
Diet
Exercise
Weight loss
Pharmacotherapy
Pharmacologic treatments are reserved for so-called metabolic derangements, such as anovulation, hirsutism, and menstrual irregularities. First-line medical therapy usually consists of an oral contraceptive to induce regular menses.
If symptoms such as hirsutism are not sufficiently alleviated, an androgen-blocking agent may be added. First-line treatment for ovulation induction when fertility is desired are letrozole or clomiphene citrate.
Medications used in the management of PCOS include the following:
Oral contraceptive agents (eg, ethinyl estradiol, medroxyprogesterone)
Antiandrogens (eg, spironolactone, leuprolide, finasteride)
Hypoglycemic agents (eg, metformin, insulin)
Selective estrogen receptor modulators (eg, clomiphene citrate)
Topical hair-removal agents (eg, eflornithine)
Topical acne agents (eg, benzoyl peroxide, tretinoin topical cream (0.02–0.1%)/gel (0.01–0.1%)/solution (0.05%), adapalene topical cream (0.1%)/gel (0.1%, 0.3%)/solution (0.1%), erythromycin topical 2%, clindamycin topical 1%, sodium sulfacetamide topical 10%)
Surgery
Surgical management of PCOS is aimed mainly at restoring ovulation. Various laparoscopic methods include the following:
Electrocautery
Laser drilling
Multiple biopsy
See Treatment and Medication for more detail.