
Practice Essentials
Exercise-induced asthma is a condition of respiratory difficulty (bronchoconstriction) that is related to histamine release,
is triggered by aerobic exercise, and lasts several minutes. Causes include medical conditions, environmental factors, and medications.
The image below illustrates the pathogenesis of asthma.
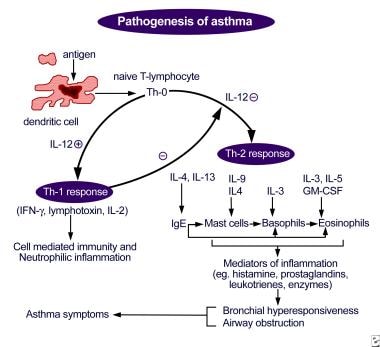
Pathogenesis of asthma. Antigen presentation by the dendritic cell with the lymphocyte and cytokine response leading to airway inflammation and asthma symptoms.
Signs and symptoms
Symptoms of exercise-induced asthma during or following exercise include the following
:
Chest tightness or pain
Cough, shortness of breath, wheezing
Underperformance or poor performance on the field of play
Fatigue, prolonged recovery time
Gastrointestinal discomfort
See Clinical Presentation for more detail.
Diagnosis
The patient’s physical examination is often unremarkable in the clinical setting but may have a higher yield on the field or after an exercise challenge.
Examination should include the following areas:
Skin: Note any signs of atopic disease
Head, ears, eyes, nose, and throat: Note any evidence of acute infection, chronic infection, or allergic/atopic disease
Pharynx: Note any mucus, cobblestoning, and/or erythema
Nose: Note presence of enlarged turbinates, erythema, and/or congestion
Sinuses: Note presence of tenderness
Lungs: Note presence of rales, rhonchi, wheezes, and/or prolonged expiratory phase
Heart: Note presence of murmurs and/or an irregular rhythm
Laboratory tests
Exercise-induced asthma is generally a clinical diagnosis. Laboratory evaluation is usually reserved for equivocal cases, for treatment failures, and to narrow the differential diagnosis.
Laboratory studies used to assess for allergy and infection include the following:
Complete blood count: To determine likelihood of infection and to evaluate eosinophil counts (for allergy)
Immunoglobulin E levels, with/without nasal swab for eosinophils: To determine likelihood of allergic disease
Skin allergen testing/radioallergosorbent test: To help identify specific allergens
Erythrocyte sedimentation rate or C-reactive protein levels: To evaluate for inflammatory and infectious conditions
Sputum analysis and culture: To help identify presence of infection and treatment options for strains of resistant organisms
Thyroid function tests: To evaluate for thyroid dysfunction if anxiety is suspected of mimicking asthma symptoms
Challenge testing to formalize the diagnosis of exercise-induced asthma includes the following:
Treadmill exercise challenges with preexercise and postexercise pulmonary function levels
Informal exercise challenge: Substitutes for treadmill exercise challenge; heart rate not monitored, and level of work not reliable
Pulmonary function testing: To evaluate baseline pulmonary function or allergic asthma; to categorize pulmonary function as obstructive or restrictive disease
Bronchoprovocation testing: Positive results indicative of general asthma rather than specific for exercise-induced asthma
Eucapnic voluntary hyperventilation: Sensitive and accurate for diagnosis of exercise-induced asthma
; can be applied in a laboratory setting and altered to mimic the environmental conditions of the patient’s specific sport
Imaging studies
Imaging studies are often not indicated in the evaluation of routine exercise-induced asthma. However, the following radiologic studies may be useful for assessing other possibilities in the differential diagnosis:
Chest radiography: To evaluate for signs of chronic lung disease (eg, hyperexpansion, scarring, fibrosis, hilar adenopathy), for congestive heart failure and/or valvular heart disease (eg, chamber enlargement, pulmonary edema, vascular or valvular calcification), and for a foreign body
Lateral neck radiography/soft-tissue penetration: To evaluate the upper airway for a foreign body or obstruction
Echocardiography: To evaluate for cardiac valvular abnormality or global contractile function, as well as dysrhythmia, cardiomegaly, or other heart disease that may manifest during exercise
Procedures
Laryngoscopy can be performed to evaluate for foreign body or other obstruction in the upper airway. Postexercise laryngoscopy can be used to evaluate for vocal cord dysfunction, a condition often mistaken for exercise-induced asthma.
See Workup for more detail.
Management
Treatment of the athlete who is experiencing an acute attack of exercise-induced asthma is the same as in any asthma attack situation and includes immediately removing the patient from competition or play.
The optimal treatment for exercise-induced asthma is to prevent symptomatic onset. After controlling the patient’s underlying and contributing factors (eg, respiratory infection, allergy, allergic asthma), a combination of drugs can be used to prevent this condition.
Pharmacotherapy
The basis of treatment for exercise-induced asthma is with preexercise short-acting beta2-agonist administration.
There is less of a role for traditional asthma medications (eg, corticosteroids, theophylline) in managing pure exercise-induced asthma.
The following medications are used in the treatment of exercise-induced asthma:
Short-acting beta2-adrenergic agonists (eg, albuterol, pirbuterol, levalbuterol)
Long-acting beta2-adrenergic agonists (eg, salmeterol, formoterol)
Mast cell stabilizers (eg, cromolyn sodium)
Inhaled corticosteroids (eg, flunisolide, beclomethasone dipropionate, ciclesonide, fluticasone, budesonide)
Xanthine derivatives (eg, theophylline)
Leukotriene receptor antagonists (eg, zafirlukast, montelukast)
5-Lipoxygenase inhibitors (eg, zileuton)
Adrenergic agents (eg, epinephrine)
Other approaches
Nonpharmacologic measures in the treatment of exercise-induced asthma include the following:
Sports selection
Altering breathing techniques (eg, predominant mouth breathing to nasal breathing)
Coordination and timing of warm-up techniques, medication, and competition
See Treatment and Medication for more detail.