
Practice Essentials
In hemorrhagic stroke, bleeding occurs directly into the brain parenchyma. The usual mechanism is thought to be leakage from small intracerebral arteries damaged by chronic hypertension. The terms intracerebral hemorrhage and hemorrhagic stroke are used interchangeably in this article and are regarded as separate entities from hemorrhagic transformation of ischemic stroke. See the image below.
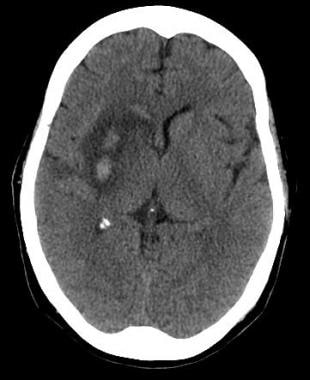
Axial noncontrast computed tomography scan of the brain of a 60-year-old man with a history of acute onset of left-sided weakness. Two areas of intracerebral hemorrhage are seen in the right lentiform nucleus, with surrounding edema and effacement of the adjacent cortical sulci and right sylvian fissure. Mass effect is present upon the frontal horn of the right lateral ventricle, with intraventricular extension of the hemorrhage.
See Acute Stroke, a Critical Images slideshow, for more information on incidence, presentation, intervention, and additional resources.
Also, see the Vertigo: 5 Case-Based Diagnostic Puzzles slideshow to help recognize diagnostic clues in vertigo cases.
Signs and symptoms
Patients with intracerebral bleeds are more likely than those with ischemic stroke to have headache, altered mental status, seizures, nausea and vomiting, and/or marked hypertension. Even so, none of these findings reliably distinguishes between hemorrhagic and ischemic stroke.
Focal neurologic deficits
The type of deficit depends on the area of brain involved. If the dominant (usually the left) hemisphere is involved, a syndrome consisting of the following may result:
Right hemiparesis
Right hemisensory loss
Left gaze preference
Right visual field cut
Aphasia
Neglect (atypical)
If the nondominant (usually the right) hemisphere is involved, a syndrome consisting of the following may result:
Left hemiparesis
Left hemisensory loss
Right gaze preference
Left visual field cut
See Clinical Presentation for more detail.
Diagnosis
Laboratory tests should include a complete blood count (CBC), a metabolic panel, and—particularly in patients taking anticoagulants—coagulation studies (ie, prothrombin time or international normalized ratio [INR] and an activated partial thromboplastin time).
Brain imaging is a crucial step in the evaluation of suspected hemorrhagic stroke and must be obtained on an emergent basis. Brain imaging aids diagnosing hemorrhage, and it may identify complications such as intraventricular hemorrhage, brain edema, or hydrocephalus. Either noncontrast computed tomography (NCCT) scanning or magnetic resonance imaging (MRI) is the modality of choice.
See Workup for more detail.
Management
The treatment and management of patients with acute intracerebral hemorrhage depends on the cause and severity of the bleeding. Basic life support, as well as control of bleeding, seizures, blood pressure (BP), and intracranial pressure, are critical. Medications used in the treatment of acute stroke include the following:
Anticonvulsants – To prevent seizure recurrence
Antihypertensive agents – To reduce BP and other risk factors of heart disease
Osmotic diuretics – To decrease intracranial pressure in the subarachnoid space
A potential treatment for hemorrhagic stroke is surgical evacuation of the hematoma. However, the role of surgical treatment for supratentorial intracranial hemorrhage remains controversial. Outcomes in published studies are conflicting.
Endovascular therapy using coil embolization, as an alternative to surgical clipping, has been increasingly employed with great success, although controversy still exists over which treatment is ultimately superior.
See Treatment and Medication for more detail.