
Background
More than 20 million people in the United States have myopia between 1.00 and 3.00 diopters (D) with astigmatism of 1.00 D or less. Several options for visual rehabilitation are available to each individual, including spectacle correction, contact lens fitting, refractive keratotomy (RK), photorefractive keratectomy (PRK)
, laser-assisted in situ keratomileusis (LASIK)
, and intracorneal rings, as shown below.
Currently, nonsurgical approaches are still the least expensive and safest. For the subset of patients who desire freedom from glasses and lenses, refractive surgery is an option.
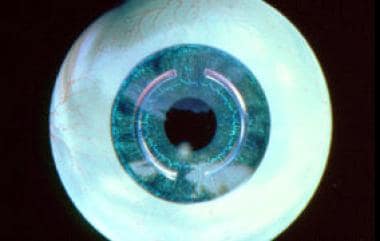
Graphic representation of the intracorneal ring segments in place. Reprinted with permission of Addition Technology Inc.

Intacs microthin prescription inserts treat mild myopia. Reprinted with permission of Addition Technology Inc.
The ideal refractive surgery procedure is one that is effective, predictable, safe, and potentially reversible.
The goal of this article is to present a refractive surgical procedure in which implantation of a polymethyl methacrylate (PMMA) ring or ring segments in the peripheral corneal stroma is used to correct myopia and astigmatism.
What initially was limited to the correction of myopia and astigmatism is now being primarily used for the management of postrefractive laser surgery associated corneal ectasia and keratoconus.
Device description
The intrastromal corneal ring (ICR) is a device designed to correct mild-to-moderate myopia by flattening the anterior corneal curvature without encroaching on the visual axis. The device is an open-ended PMMA transparent ring with an outer diameter (R2) of 8.1 mm and an inner diameter (R1) of 6.8 mm, and the curvature conforms to that of the cornea. It is precision lathe-cut to ±0.01 mm as a hexagonal-shaped section of a cone with positioning holes for manipulation.
It is inserted through a peripheral radial incision made with a diamond knife at two-thirds corneal depth in to a 360° peripheral intrastromal channel created with specially designed instruments. Anterior corneal curvature is changed by using rings of different thicknesses.
Intrastromal corneal ring segments (Intacs microthin prescription inserts, as shown below), or ICRS, are a more recent design modification of the ICR. The ring segments split the ring into two 150° arcs.
The use of ring segments simplifies the implantation procedure. Furthermore, ring segments can be placed away from the radial incision, thereby minimizing the potential for incision-related complications. The degree of correction (greater-thicker) is determined by the thickness of the Intacs inserts, which are available in 5 sizes: 0.25 mm, 0.275 mm, 0.30 mm, 0.325 mm, and 0.35 mm.

KeraVision Intacs microthin prescription inserts. Reprinted with permission of Addition Technology Inc.

KeraVision Intacs microthin prescription inserts. Intracorneal ring segments. Reprinted with permission of Addition Technology Inc.
MediPhacos KeraRing is another intracorneal ring segment developed and marketed in Brazil. It is available in 2 models for 5-mm implantation in optical zones of 5 mm, 5.5 mm, and 6 mm. There are 40 different variations of thicknesses, arc lengths, and diameters, allowing for enhanced customization of corneal remodeling and refractive correction. Over 150,000 implants have been used worldwide.
Ferrara Ring is made of yellow PMMA, an inert and biocompatible acrylic used in intracorneal implants. The apical diameters are 5 mm and 6 mm. It has a flat base with a variable arch length of 90 mm and 210 mm and a variable thickness of 0.15 mm to 0.30 mm.
Surgical instruments
Addition Technology has surgical instruments specifically for use with Intacs insertion. These instruments include the following: corneal thickness gauges, glides, incision and placement marker, pocketing hook, pocketing lever, ring forceps, stromal spreader, vacuum-centering guide with vacuum system, and clockwise and counterclockwise dissectors.
Ferrara Ring has its own surgical kit used in the insertion of the intracorneal ring segments. These instruments include the following: Ferrara spatula, Suarez spreader, Bicalho guide, Pre-delaminator, Ferrara marker, Sinskey hook of 0.20 mm, Modified McPherson forceps, and an adjustable Ferrara diamond blade knife.
How do intracorneal ring segment inserts work?
Imagine the cornea as compressed arcs of fiber covering the eye. If a spacer element is inserted between those fibers, effectively pushing them apart, then the arc must flatten to accommodate the inserted element. The corneal ring complies with Barraquer and Blavatskaya postulates. According to these postulates, an addition in the cornea periphery results in its flattening, and the ring diameter determines how much the cornea will be flattened. In other words, the more tissue is added (increasing ring thickness) and the smaller the diameter, the greater will be the myopia correction obtained. Intracorneal ring segments inserts shorten the corneal cord length, produce flattening across the entire cornea, and maintain the positive asphericity of the cornea.
Advantages of intracorneal ring segment inserts
Several benefits of using intracorneal ring segment inserts exist. It is a minimally invasive outpatient procedure with low morbidity. Since the surgery is completed in the peripheral cornea, the central optical zone is not disturbed. Results are rapid and predictable. There is a reduced risk of visual adverse effects and a long-term convenient refractive correction. It is removable and exchangeable. There is central and peripheral flattening of the cornea, maintaining corneal asphericity (prolate).
Intracorneal ring segments may now be used to treat irregular steepening (irregular astigmatism) of the cornea caused by keratoconus.
There is a stabilization or delay of cone progression. The intracorneal ring segment is made of acrylic, an inert and biocompatible material; therefore, there is lack of rejection. There is a high patient satisfaction rate. It is possible to combine with other procedures like contact lens fitting, corneal collagen cross-linking, PRK, phakic IOL implantation, and intraocular lenses. There is no evidence of any interference with a corneal transplant.
Disadvantages of intracorneal ring segment inserts
The technology is limited for use in low-to-moderate myopia with low astigmatism, corneal ectasia, and keratoconus.
It is still a relatively new technology with emerging complications (eg, diurnal fluctuations in visual acuity, stromal opacifications).
Of further concern is the prolonged intraoperative elevated intraocular pressure.