
Practice Essentials
Progressive supranuclear palsy (PSP) is a neurodegenerative disease (see the image below) whose characteristics include supranuclear, initially vertical, gaze dysfunction accompanied by extrapyramidal symptoms and cognitive dysfunction. The disease usually develops after the sixth decade of life, and the diagnosis is purely clinical.
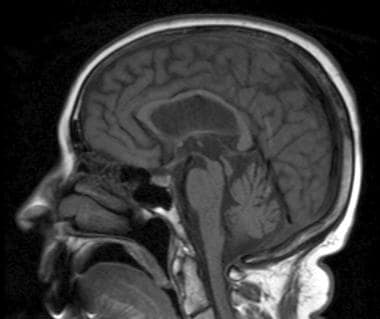
Sagittal T1-weighted image shows atrophy of midbrain, preservation of pontine volume, and atrophy of the tectum, suggestive of progressive supranuclear palsy (Steele-Olszewski-Richardson disease).
Signs and symptoms
The onset of PSP is insidious and usually includes a prolonged phase marked by the following symptoms:
Fatigue
Headaches
Arthralgias
Dizziness
Depression
Patients also experience subtle personality changes, memory problems, and pseudobulbar symptoms, which are often more evident to the family than to the patient. The initial symptoms can often involve unexplained imbalance or falls.
The cardinal manifestations of PSP are as follows:
Supranuclear ophthalmoplegia
Pseudobulbar palsy
Prominent neck dystonia
Parkinsonism
Behavioral, cognitive, and gait disturbances that cause imbalance
Frequent falls/impaired postural reflexes
Findings on physical examination can include the following:
Poor postural reflexes, axial rigidity greater than appendicular rigidity, and dysarthria (monotone with slight hypophonic quality)
Absence of cogwheeling or tremor
Widely based and unstable gait
Bradykinesia with masked facies and a startled expression
Retrocollis may be present
Visual signs and symptoms
Slow vertical saccades and square wave jerks on ocular examination (early signs)
Supranuclear ophthalmoplegia (classic gaze palsy in PSP)
Downgaze typically involved before upgaze
Improvement in supranuclear vertical gaze limitation after extravolitional pathway activation with the vestibular ocular reflex (VOR) or the Bell phenomenon
Nearly continuous square wave jerks commonly observed with fixation
Impairment of convergence eye movements (may cause diplopia)
Eyelid retraction, eyelid opening or closing apraxia, blepharospasm, or lid lag
Complete ophthalmoparesis in advanced PSP
Cognitive symptoms
Slowed cognitive processing, sequencing and planning difficulties, mild memory difficulty, and apathy (generally more prominent in late disease)
High apathy scores coupled with low agitation and anxiety scale scores on Neuropsychiatric Inventory testing
See Clinical Presentation for more detail.
Diagnosis
The diagnosis of PSP is clinical. Key features typically develop over time. Participants in a National Institute of Neurological Disorders and Stroke (NINDS)/Society for PSP conference have formulated and validated clinical research criteria for the diagnosis of PSP.
In this system, criteria for possible PSP are as follows:
Gradually progressive disorder with onset at age 40 years or older
Either vertical supranuclear palsy or both slowing of vertical saccades and prominent postural instability with falls in the first year of onset
No evidence of other diseases that can explain the clinical features
Criteria for probable PSP are vertical supranuclear palsy with prominent postural instability, falls in the first year of onset, and other features of possible PSP, as follows:
Abnormal neck posture, especially retrocollis
Poor or absent response of parkinsonism to levodopa therapy
Early dysphagia and dysarthria
Early cognitive impairment with at least 2 of the following: apathy, abstract thought impairment, decreased verbal fluency, imitation behavior, or frontal release signs
Criteria for definite PSP are as follows:
History of probable or possible PSP
Histopathologic evidence that is typical of the disease
The workup in patients with suspected PSP is directed principally at eliminating other diagnoses (eg, Whipple PCR to eliminate possible Whipple disease). MRI offers little help in the early stages of PSP, but may reveal the following abnormalities in some advanced cases
:
Atrophy of the midbrain (see the image below) with cisternal and ventricular dilatation
Thinning of the quadrigeminal plate
Dilation of the third ventricle
A nonspecific finding of increase in proton density images in the periaqueductal gray matter, compatible with gliotic changes
Sleep studies in patients with PSP show the following abnormalities, although these are not specific for PSP:
Diminished total sleep time
Increased awakenings
Progressive loss of rapid-eye-movement (REM) sleep
Decreased REM–to–non-REM (NREM) quotient
See Workup for more detail.
Management
No medication is effective in halting the progression of PSP; however, medications that may provide modest symptomatic improvement include the following:
Dopamine agonists
Tricyclic antidepressants
Methysergide
OnabotulinumtoxinA: May be useful for rigidity (nuchal rigidity in particular) and dystonia (eg, blepharospasm, bruxism, and focal limb dystonia)
Methylcellulose or methyl alcohol eyedrops: For relief of chronic conjunctivitis from reduced blink rate
Physical therapy and rehabilitation medicine involvement may help maximize ambulation safety and facilitate instruction in the use of a walker, wheelchair, or other aids.
See Treatment and Medication for more detail.