
Background
Cholesterol embolism, or atheroembolism, is a condition that has historically been a diagnostic challenge owing to its nonspecific symptoms and because it often mimics other more common conditions and diseases. Autopsy studies have revealed that up to 15-20% of individuals older than 60 years with a history of atherosclerosis had cholesterol emboli present, which suggests that cholesterol embolism may be more frequently undiagnosed than originally believed.
Cholesterol embolism is categorized as a disorder of occlusion due to emboli, wherein there is luminal obstruction of small- and medium-caliber arteries (100-200 μm in diameter) by cholesterol crystals (see the image below) that form from fragmentation of ulcerated atheromatous plaques inside vasculature. Although it was initially reported by Panum over a century ago, the diagnosis of cholesterol embolism is often missed or overlooked, resulting in potentially devastating and even fatal consequences. In 1987, Fine et al. described certain hallmark skin findings in patients with cholesterol embolism, thereby linking cholesterol embolism to recognizable signs and symptoms that could be identified clinically.
In 1999, Belenfant et al reported new treatment regimens for the management of cholesterol embolism, allowing for breakthrough advances in patients with this disease.
Despite these medical developments, cholesterol embolism remains a challenging entity to accurately diagnose and effectively treat. Numerous comorbid conditions can be associated with the development of cholesterol embolism, including hypertension, hyperlipidemia, diabetes mellitus, peripheral vascular disease, and tobacco use.
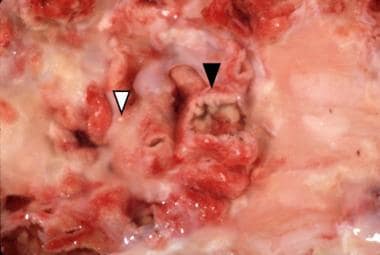
Aorta with an ulcerated plaque (black arrowhead) on the luminal side photographed under water to enhance reflection of cholesterol crystals (white arrowhead).
A high index of suspicion is imperative because the signs and symptoms of cholesterol embolism are often atypical, unrecognized, not temporally correlated with the onset of physical findings, and/or simply overlooked. Unfortunately, there is no laboratory testing that is specific for cholesterol embolism, although serologic markers checking for eosinophilia and inflammation may be helpful.
Additionally, diagnosis is suggested by progressive increases in blood urea nitrogen and creatinine levels following an invasive arterial procedure. On physical examination, the presence of netlike or lacelike, bluish to deep-purple patches with a mottled appearance involving the distal extremities and blue fingers or toes can be invaluable clinical features in diagnosing cholesterol embolism (see the image below). On pathology, cholesterol embolism can be identified by characteristic needle-shaped cholesterol clefts and intravascular microthrombi; however, one or both of these findings may be absent and do not necessarily correlate directly with a patient’s clinical disease.

Symmetric involvement of the feet with livedo reticularis on the plantar surface of the forefoot and cyanosis of the left fifth toe. The painful cyanotic toe is typical of blue toe syndrome.